
Your skin at 35 doesn’t age like it does at 55. That difference determines whether you’re spending money on the right treatment or wasting it on something that won’t work for what’s actually happening beneath your skin.
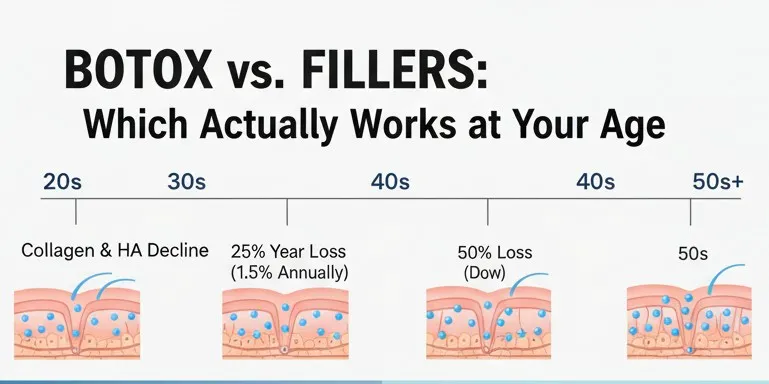
Collagen production drops 1-1.5% every year after 30. By the time you hit 50, you’ve lost roughly half your collagen stock. A study tracking 389 women between ages 27-74 found that optimal Botox dosing varies wildly by age—younger patients needed 15% higher forehead doses while older patients required 30% more around the eyes.
What Changes as You Age
Skin stiffness measurements tell the real story:
- Young adult skin: 4.9 kPa
- Age 60 skin: 1.6 kPa (67% reduction)
- Hyaluronic acid levels: Drop 50% by age 50
These numbers explain why Botox alone stops working as well after 40. When you relax facial muscles in young skin with intact collagen, the skin springs back smooth. In older skin with 40% collagen loss, relaxing muscles just creates flatness. The underlying volume deficit stays untouched.

Treatment Results by Age Group
| Age Group | Botox Procedures Annually | Filler Procedures Annually | What This Tells You |
| 20-29 | 143,000 | Growing 32% | Mostly preventative, often unnecessary |
| 30-39 | 1.82 million | 608,000 | Botox dominates—volume loss hasn’t hit yet |
| 40-54 | 5.62 million | 2.68 million | Largest market—both treatments needed |
| 55-69 | 2.27 million | 1.89 million | Pattern reverses—volume restoration matters more |
The 40-54 age group dominates both markets because this decade requires comprehensive strategies. By your 40s, you’ve lost about 25% of total collagen from peak levels, creating visible volume deficits that Botox can’t address.
Your 30s: Botox Works, Fillers Usually Don’t
Clinical trials examining adults under 41 showed that 86-87% achieved visible wrinkle improvement with Botox, maintaining results for 150-180 days. Volume loss hasn’t hit yet. Most filler use in this decade focuses on enhancement like lip augmentation rather than replacing lost structure.
Filler duration peaks now:
12-18 months in your 30s compared to just 6-9 months in your 40s. Preserved collagen levels between 70-85% of peak mean fillers integrate better and stay put longer.
Starting Botox in early-to-mid 30s offers preventative benefits. Once you hit 35, the strategy shifts from preventing lines to correcting them. After lines become static—visible even when your face is relaxed—Botox alone provides limited help.
This age group showed 16.4% adverse event rates compared to 13.3% in older patients—mostly headaches from the higher doses needed for stronger muscles.
Your 40s: The Crossover Point
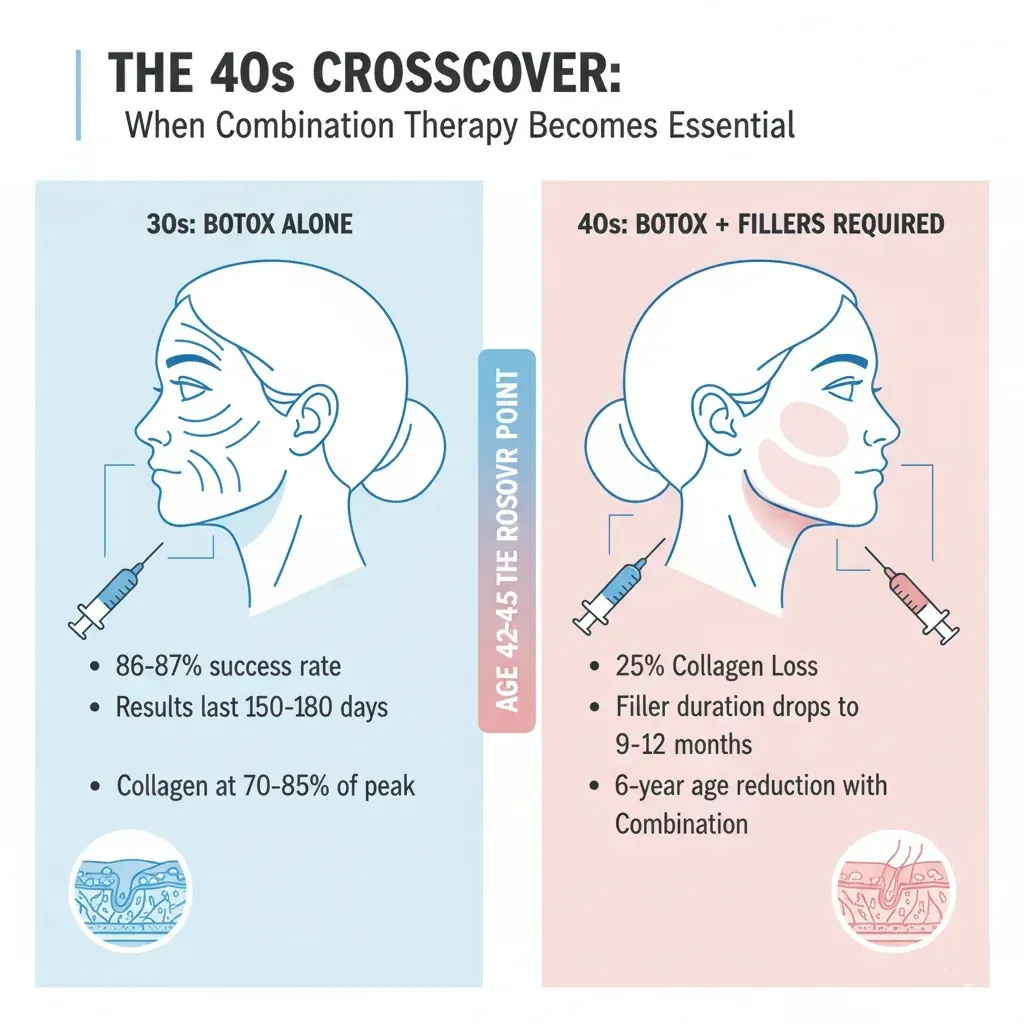
Around age 42-45, something shifts. Patients who achieved excellent results with Botox alone in their 30s start noticing it doesn’t work the same way. Lines smooth during treatment but the overall face looks somehow less full, less lifted.
Research on combined treatments found that each additional modality produced statistically significant improvements. Case series data showed patients in their early 40s achieved 6-year apparent age reductions with combination treatments, while those in late 30s achieved only 4-year reductions.
What’s changing biologically:
- Lost approximately 25% of total collagen from peak levels
- Filler longevity decreases substantially (9-12 months vs 12-18 months in 30s)
- Collagen turnover rates decline
- Fibroblast function reduces—cells producing collagen drop from 78% to 58% surface attachment
Dosing patterns shift: Patients over 50 required 30% higher periorbital Botox doses to achieve equivalent results, while forehead doses decreased 12-15% per decade. Increased muscle recruitment around the eyes compensates for lost structural support underneath.
Your 50s and Beyond: Volume Takes Priority
A counterintuitive finding: A 57-year-old achieved 8 years of apparent age reduction from combination treatments, while a 69-year-old achieved 14 years—double the 4-6 years seen in patients in their 40s. This reflects the substantial volume deficit in older patients. Restoring structural foundation produces more dramatic visible improvement than fine-tuning already-adequate facial volume.
By 50-plus, patients have lost approximately 50% of collagen stock. Postmenopausal women experience additional 2.1% annual decline for 15-18 years. Aged fibroblasts produce 32% less type I collagen.
Filler duration shortens: 6-12 months for hyaluronic acid products due to compromised extracellular matrix and faster enzymatic degradation. However, MRI studies revealed that fillers persist far longer than clinically visible—detected 2-5 years post-injection in 21 patients and beyond 5 years in 12 patients. Some showed residual filler 8-15 years later.
The 55-69 age group shows preference for longer-lasting non-hyaluronic acid fillers like Sculptra and Radiesse rather than standard hyaluronic acid products.
Critical dosing consideration: Excessive Botox in patients over 60 with reduced muscle mass risks accelerating an atrophic, hollow appearance—the opposite of desired rejuvenation. Conservative dosing that modulates rather than paralyzes muscles becomes essential, with starting doses 20-30% lower than for middle-aged patients.
How Long Results Actually Last
- Botox duration: Remains relatively stable at 3-4 months across age groups. The drug’s systemic half-life stays consistent at 3.8-4.3 hours. Maintenance schedules stay consistent every 3-4 months regardless of age.
- Annual Botox cost: $1,740-$2,120 yearly at average prices of $435-$530 per treatment (3-4 sessions).
Filler longevity by age:
| Age Range | Hyaluronic Acid Duration | Collagen-Stimulating Fillers |
| 20s-30s | 12-18 months | Up to 24 months |
| 30s-40s | 9-12 months | Up to 18 months |
| 40s-50s | 6-9 months | Up to 12 months |
| 50s+ | 6-12 months | 12-18 months |
This progressive shortening reflects declining collagen synthesis rates, increased degradation of newly synthesized collagen, and compromised tissue structure providing less mechanical support.
Annual filler maintenance costs:
- 20s: $500-$1,500 for targeted treatments
- 30s: $2,000-$4,000 for balanced approaches
- 40s-50s: $3,000-$7,000+ for comprehensive protocols
Treatment Timing: Sequence Matters
Multiple studies recommend injecting Botox first, then waiting 2-4 weeks before adding fillers. This creates a relaxed muscular framework that enhances filler longevity by reducing mechanical stress from muscle contraction. The sequence improves distribution, increases satisfaction, and reduces total filler volume needed.
Safety Track Record by Age
Botox demonstrates superior safety across all age groups for cosmetic use:
- Serious adverse event rates: Below 0.01% for Botox vs 0.1-1% for dermal fillers
- Adverse events remain mild across ages
- Injection site reactions, bruising, and headache comprise 90-95% of all reports
- Eyelid drooping occurs in 1-5% of cases (20% with forehead injections)
FDA surveillance of 1,437 adverse event reports revealed that therapeutic Botox use showed 33-fold higher serious complication rates than cosmetic use—attributed to higher doses and complicated underlying neurological diseases rather than inherent product risk.
Elderly patient considerations:
- Delicate skin increases bruising
- Reduced orbital septum heightens drooping risk
- Polypharmacy creates interaction potential (aminoglycosides and anticholinesterases potentiate Botox effects)
- Conservative dosing starting 20-30% lower becomes essential
Dermal filler safety: Mean age of filler complications ranges 34-50.9 years across studies, with 88.9% occurring in women. Vascular occlusion leading to tissue necrosis or blindness represents the most serious risk—approximately 190 cases of filler-induced blindness reported historically. Incidence remains exceedingly rare at approximately 0.001%.
Age-related filler considerations in older patients: Thinner, more fragile skin increases bruising and migration risk. Anticoagulant medication use heightens bleeding complications. Preexisting vascular disease elevates occlusion risk.
Recovery time shows minimal age variation—immediate swelling lasts 3-7 days, bruising resolves within 7-14 days, full results visible at 2-3 weeks.
What to Do at Each Age
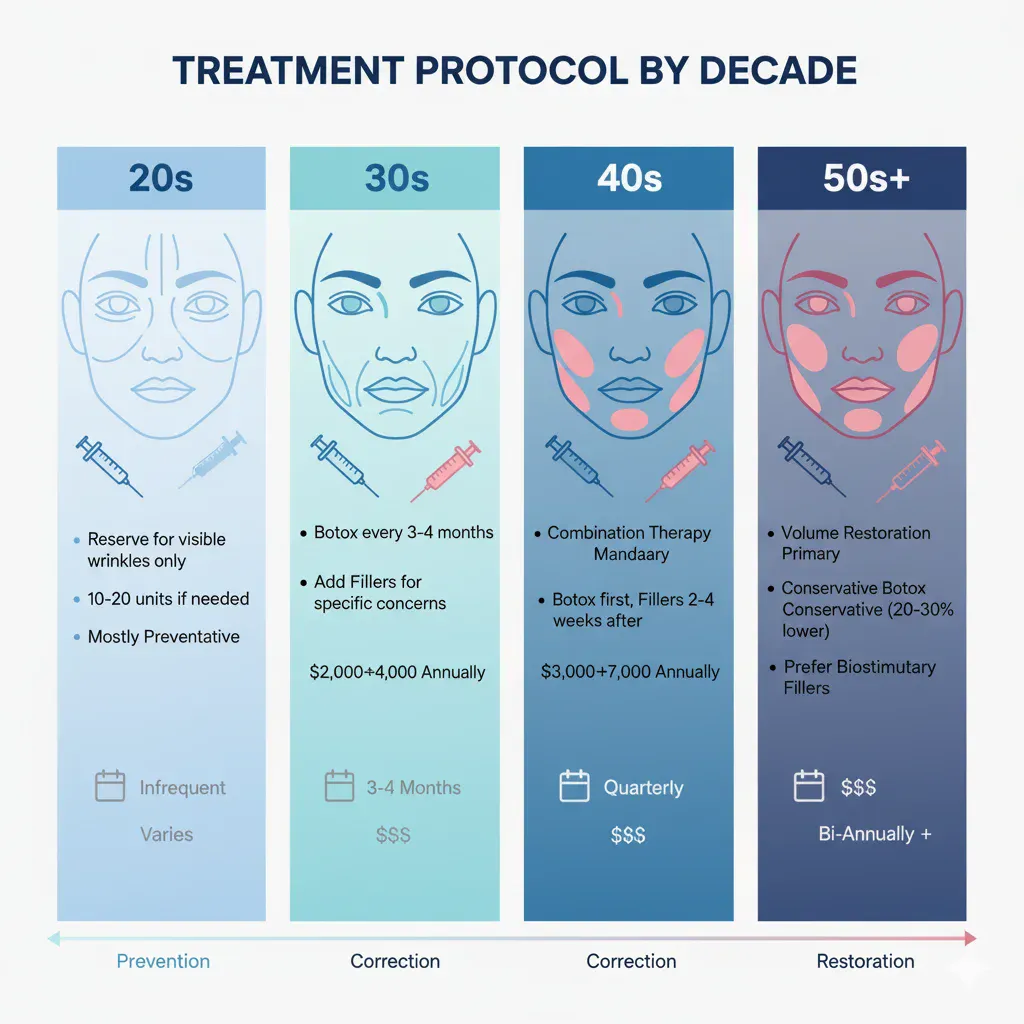
- Ages 20-29: Reserve treatment for visible dynamic wrinkles. Avoid procedures if lines only appear during expressions. Conservative doses of 10-20 units per area if indicated. Fillers typically inappropriate unless for enhancement goals.
- Ages 30-39: Standard preventative Botox when lines persist at rest. Typical treatment areas include forehead, glabella, and crow’s feet. Maintenance every 3-4 months. Add fillers only for specific concerns like tear troughs or early nasolabial folds. Focus on prevention while skin retains structural integrity.
- Ages 40-49: Mandatory combination therapy for comprehensive rejuvenation. Botox addresses upper face dynamic wrinkles while fillers restore midface volume. Sequential protocol recommended: Botox first, wait 2-4 weeks, then strategic filler placement. Consider collagen-stimulating fillers for longer-lasting results.
- Ages 50+: Volume restoration becomes primary goal. Comprehensive filler plan for multiple facial zones with selective Botox only where muscle hyperactivity persists. Excessive Botox in elderly patients risks accelerating hollowed appearance. Prefer longer-lasting biostimulatory fillers to minimize treatment frequency.
Why This Works: The Biology
Botox works by blocking acetylcholine release at the neuromuscular junction, preventing muscle contraction visible 3-5 days post-injection. This effect is entirely collagen-independent—efficacy depends on muscle activity, not structural support. In young skin with predominantly dynamic wrinkles and intact collagen networks at 70-100% of peak, the tissue springs back when muscles relax.
In aged skin with greater than 40% collagen loss, static wrinkles present at rest cannot improve from muscle relaxation alone. Fragmented collagen matrix lacks mechanical tension to recoil. Volume deficits remain unfilled. Botox used alone in severely aged skin may worsen appearance by creating flatness without addressing underlying structural deficit.
Dermal fillers work through direct volume replacement and fibroblast activation. Hyaluronic acid fillers immediately fill space left by collagen depletion, binding 1000 times their volume in water to restore hydration. Cross-linked particles also mechanically stretch the extracellular matrix, activating fibroblast receptors to stimulate signaling pathways.
Collagen-stimulating fillers like poly-L-lactic acid increase collagen deposition via specific immune responses, with effects lasting 24+ months. Calcium hydroxylapatite provides immediate volume while stimulating new collagen over months. These mechanisms explain why fillers work increasingly well in older patients: the more severe the structural deficit, the more dramatic the improvement from restoring that foundation.
The biological synergy of combination therapy addresses both causes. Botox reduces ongoing collagen damage from muscle activity while smoothing remaining dynamic wrinkles. Fillers replace lost volume, stimulate fibroblast activity, and provide scaffolding for Botox results. Together they prevent future aging while correcting existing damage—optimizing outcomes neither achieves alone.
The Evidence Gap You Should Know About
According to analysis by Dr. Anne Therese Stubbs MD from www.annetherese.com and synthesizes data from FDA post-marketing surveillance tracking thousands of adverse events, professional society statistics covering millions of annual procedures, systematic reviews of randomized controlled trials, and large retrospective patient cohorts. The biological data comes from peer-reviewed studies measuring collagen production rates, skin elasticity changes, and cellular function across age groups.
But no high-quality randomized controlled trials directly compare Botox versus dermal fillers with age-stratified primary endpoints. Existing studies examine products individually, combined treatments without comparative analysis, or post-hoc age subgroups within broader trials. Only two trials included age-matched cohort analyses.
The evidence base consists primarily of retrospective cohort studies, small prospective case series, expert consensus statements, and demographic surveys rather than rigorous comparative trials. Patient satisfaction scores are rarely reported separately by age group.
This gap stems from practical realities. Botox and fillers address fundamentally different aging mechanisms—muscle hyperactivity versus volume loss—making direct comparison scientifically problematic except in combination therapy studies.
Current recommendations rely heavily on extrapolated data and clinical consensus rather than Level 1 evidence. That doesn’t invalidate the guidance—expert consensus based on decades of clinical experience and thousands of patients provides valuable direction. But definitive answers about which treatment works better at specific ages remain incomplete.
Matching Biology to Treatment
Age-specific treatment selection fundamentally rests on understanding which biological aging mechanism predominates:
- 30s: Muscle hyperactivity creates dynamic wrinkles in skin with preserved structural integrity—Botox works optimally
- 40s: Emerging collagen loss creates mixed dynamic and static wrinkles with early volume loss—combination therapy becomes essential
- 50s+: Severe structural deficits necessitate comprehensive volume restoration—fillers provide primary benefit with strategic Botox supplementation
Individual assessment matters more than chronological age alone. Some 45-year-olds have skin biology resembling a typical 35-year-old. Others show advanced aging from sun damage, smoking, or genetics.
Treating the biology rather than the birthday delivers better outcomes. Your face at 35 operates fundamentally differently than at 55—and your treatment strategy should reflect that reality.